Chisolm and Porcher during the Civil War
Anesthetics in Field and General Hospitals
Of the Confederate States of America During the Civil War
1861-1865:
The Use of Indigenous Botanical Substitutes
versus
The Availability of Chloroform
by Michael
Koznarsky, 2LT, USAF, BSC

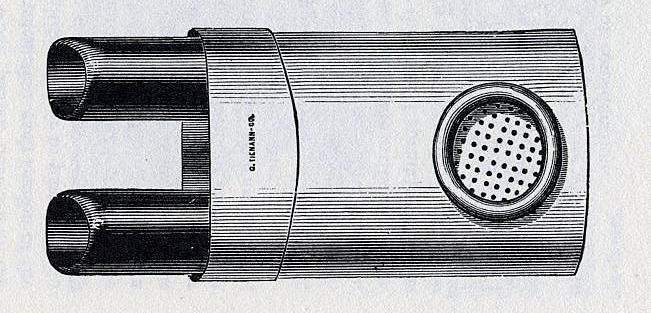
Chisolm Pocket Ether or
Chloroform Inhaler by Tiemann
The above illustration is taken
from a Tiemann catalog and is their version of the Chisolm Pocket Ether
Inhaler. The original by Chisolm was made of brass, and the body
of the container was painted black, the two parallel nasal tubes were
brass colored.. Overall size was about equal to the size of an old
Zippo-pocket lighter.
The following photos are from the
sale of a 'fake' Chisolm Pocket Ether Inhaler on eBay. The seller
admits it is a fake and a copy of the Chisolm design. The
blackened tin is correct, but this is NOT the original, but is similar
in appearance.




Please see additional information
on
ether and chloroform use during the Civil War
INTRODUCTION
Anesthetics, chiefly chloroform, ether and opium/opium
derivatives, were widely used during surgery and for pain relief
during the American Civil War. Standard medical practices of both
the United States and Confederate States called for the use of these
anesthetics. The Confederacy also strove to use indigenous botanical
substitutes for medical purposes. The use of these varied botanical
substitutes has left the impression that the South was bereft of
anesthetics, in particular chloroform, and was forced to use the
substitutes on a grand scale. This, however, is not the truth.
Southern hospitals, both field and general, were rarely without the
painkilling drug chloroform.
A wide variety of painkillers were available to the Civil War
physician but at the top of this list the surgeon of the times chose
from ether, chloroform, opium and its derivatives laudanum and
morphine. Ether and chloroform were the drugs of choice for the
initiation of surgical procedures to induce “the desired
insensibility”1, whereas all but ether were used to reduce the pain
following surgery or as a general pain reliever.2 Surgeon
J. Julian
Chisholm, M.D., professor of surgery in the Medical College of South
Carolina, stated in his book
A Manual of Military Surgery, “During
the performance of capital operations on the battlefield, death
sometimes ensues from nervous exhaustion, produced by excess
of suffering; the use of chloroform relieves the patient at least
from this risk.”3 He writes further to state, “The universal use of
chloroform to allay the pain of surgical operations, is a complete
vindication of the utility of the remedy, and proof of its
necessity... We do not hesitate to say, that it should be given to
every patient requiring a serious or painful operation.”4
INDIGENOUS BOTANICAL SUBSTITUTES
Shortly after the start of the war, Confederate Surgeon General
Samuel Preston Moore instructed Surgeon (Major)
Francis Perye
Porcher to prepare a “treatise on the resources of Southern fields
and forests” regarding the “medicinal, economical and useful
properties of the trees,
plants and shrubs” found in the Confederacy.5 Moore realized from
the beginning of the war that medical supplies would be in short
supply6; this became ever more critical when medical and surgical
appliances were named “contraband of war” by the Union government.
So important was the task of developing indigenous botanical
substitutes for drugs and medicines that he temporarily relieved
Porcher of his duties as surgeon to the Holcombe Legion. Porcher was
the obvious choice for this task having already written two
medico-botanical texts: one of the flora of South Carolina and the
other about the botanical properties of plants of the United
States.7 His new book, Resources of the Southern Fields and Forests,
Medical, Economic and Agricultural, is credited with saving “the
Confederacy for two years”.8 Published in 1863 and distributed to
medical officers, it offered about 600 pages of information on the
use of botanical substitutes for traditional medications. Moore
continually stressed the necessity of officers to collect and use
indigenous botanical substitutes for the sick and wounded.9 The
desire to produce home grown medical remedies prompted the writing
and publishing of other, similar texts during the Civil War: The
Flora of the Southern States, Chapman; Plants Growing in the
Vicinity of Charleston, Dr. J. Bachman; and Plants Found in the
Vicinity of Newbern, North Carolina, H. B. Croon.10
Surgeon General Moore was not alone in his assessment of the need to
produce and procure medical equipment and medical supplies for use
by the Confederate States. While many speculator could be commended
for his altruistic, dedicated patriotic duty, many more were driven
by greed and the ability to buy low and sell high. For instance,
Southern traders could purchase a bag of salt in the North for $1.25
and, in the South, resell it for $60, a mark up of almost 5000%!11
The activities of and
problems involved with speculation and medical goods even caught the
attention of the Commander in Chief of the Army of Northern
Virginia, General Robert E. Lee. In September 1862 he wrote to
Secretary of War George W. Randolph:
I desire to call your attention to a fact reported to me by M.
Schriver which cannot be but injurious to the service. He states
that as soon as any place is open by retreat of the enemy, before
the agents of the government can purchase such medical stores as it
requires, numbers of speculators from Richmond and other places buy
up everything at much higher prices. Mr. Schriver states that at
Fredericksburg he had the knowledge of at least 60 of this class of
persons as soon as the enemy left... I have directed that medical
stores found in the possession of such persons... shall be seized
and paid for at their cost price [and] that measures be taken to put
a stop to it and to prevent persons from coming into places vacated
from the enemy with such intentions.12
Major Porcher’s efforts were applauded in the July 1864 issue of the
Confederate States Medical and Surgical Journal . The editorial
wrote that we should not “fail here to notice the useful and
laborious effort of Surgeon Porcher, in bringing before the public
in his work on the Resources of the Southern Fields and Forests the
amount of useful material at hand.”13 In this same issue is printed
a “Standard Supply Table of the Indigenous Remedies for Field
Service and Sick in General Hospital”14, a table listing botanical
names, common names, medical properties, dosage and method for
administration. In the list of 65 plants, however, there is no
mention of a botanical substitute for chloroform and only one for
use as a sedative. A recent historian also notes that “ Generally
speaking, the Medical Corps had good preparations and few
substitutes.”15
Surgeon (Major) E. Burke Haywood, General Hospital No. 7, Raleigh,
North Carolina, references both the early and mid-war literary works
by Porcher’s in the use of Sarracencia Purpura (Side Saddle of Fly
Trap) in the treatment of small pox. Haywood notes that, although
contradictory works appear several praise its effects writing, “the
unmistakable evidence of the efficacy of this remedy in arresting
the progress of small pox has been conspicuously manifested in many
cases.”16 Although Porcher is reported to have tested the plant on
himself and writes of its widespread use in Georgia and South
Carolina, Haywood states that after procuring a supply will fully
test its efficacy and reports the results.17 Unfortunately, no such
follow up is found in the pages of the Confederate States Medical
and Surgical Journal.
In the June 1864 issue of the Confederate States Medical and
Surgical Journal, Assistant Surgeon (Captain) W. T. Grant writes an
extensive article about Indigenous Medicinal Plants. He mentions
various plants, their successful uses and where they can be found.
Of note, he mentions the poor quality and reliability of a
substitute for quinine, “nearly proved a failure.”18 The concoctions
made up as a quinine substitute were decidedly inferior.19
The use of indigenous botanical resources is thus well documented by
several independent sources in the Confederate States Medical and
Surgical Journal and appears to be in use by Southern medical
officers. Surgeon General Moore was dismayed at the failure of some
officers on the regimental level to fully utilize this
information20; he also wrote, “Our savannahs furnish our meteria
medica with a moderate number of narcotics and sedatives and an
abundant number of tonics, astringents, and demulcents...”21 Diverse
discussion is made of the efficacy of these many plant substitutes
as medicines other than as anesthetics; dissension is involved in
the case of quinine substitutes.
Perhaps one of the strongest arguments for the lack of effective
botanical substitutes for anesthetics comes from Porcher himself. In
his approximately 600 page long book of over 400 entries,22
Resources of the Southern Fields and Forests, Medical, Economic and
Agricultural, he makes but four entries for anesthetics and 28 for
narcotics. Listed are topical anesthetics (Schrankia Augusta and
Uncinata)23, cures for headaches/pain from flatulence (Solidago
Odora - Goldenrod)24, “seeds... said to induce delirium and partial
forgetfulness” (Datura Stramonium - similar to Foxglove)25 and a
powerful local drug that “produced a feeling of numbness... which
lasted a whole day” (Aconitum Uncinatum - Wolfsbane)26. The last was
touted as “no remedy, save chloroform, equals it when applied
locally for the relief of pain.”27 There are 28 different sources of
narcotics including Indian Tobacco, Bush Honey Suckle, Wild Lettuce,
Orange Root, Cannabis Sativa and the Opium Poppy.28 Contradictory
evidence surrounds the efficacy of the Southern poppy - sources can
be found that laud the Southern white or red poppy as an acceptable
source of opium; other sources report the poor quality of the
same.29
As mentioned earlier, the sources of painkillers were available to
the Civil War surgeon were ether, chloroform and opium/opium
by-products. In general, ether was the primary choice of Northern
doctors while chloroform was preferred by Southern doctors.30
Chloroform was a “remedy which the surgeon should never be
without.”31
Shortages of chloroform in Southern hospitals, frequently a matter
of feast or famine, produced many ingenious ways to use it as
economically as possible.32 Normal medical practice of the day
called for the application of the chloroform to a piece of folded
cloth or sponge, held in the apex of a funnel or cone and held a
distance from the patient’s nose so the first inhalation was well
diluted with fresh air. Creams or salves could be applied to the
nasal area to reduce the caustic and blistering effects of
the chloroform. As the patient exhaled the chloroform soaked cloth
or sponge was brought closer to the nose. Noisy breathing was the
clinical sign that inhalation should be stopped; the surgical
procedure could then commence. Longer surgeries would require
further administration of anaesthetic.33 The effects as per one of
the more famous Southern patients, General Thomas J. Jackson, was
reported as “What an infinite blessing.”34 Ingenious methods were
developed to stretch potentially scarce supplies of chloroform
including smaller inhalers that fit into the nostrils of the
patient. Surgeon J. Julian Chisholm, inventor of the two and one
half inch Chisholm inhaler, realized the savings in chloroform with
the increased risk of suffocation of the patient.35
The necessity for the use of chloroform in surgical procedures in
both the field and general hospitals was well documented and, in
general, agreed upon. The preference of chloroform over ether has
been previously discussed. Southern pharmaceutical companies, almost
nonexistent at the start of the war 36, developed to a point where
in 1864 it was reported that, “A most gratifying progress has been
made in the manufacture of chemicals within our own limits...
Botanical Gardens and farms are flourishing... Manufactories and
laboratories are flourishing at various points.”37 Very specific
reference is made to the various drugs produced, however, no mention
is made of anesthetics. In fact, Charles Theodore Mohair, reportedly
one of the ablest druggists in the Confederacy, describes one of his
tasks as examining the medical supplies smuggled from Europe,
including opium, morphine, quinine and others.38 In all of the
literature
there are no references to the use of indigenous botanical
substitutes for anesthetic purposes. Further, no information was
located in general hospital or regimental sources of the use of any
plant or flora substitute for chloroform. With all of this in mind,
how did the Confederate purveyors, the procurers of medical supplies
for both field and general hospitals, supply the rebel armed forces
with the vital chloroform the surgeons and the wounded required?
SOURCES OF CONFEDERATE CHLOROFORM
The Confederate medical organization was supplied of chloroform from
three major sources: 1) through
blockade running, 2) by smuggling through Union lines and 3) from
captured Union supplies. Blockade
running in the early part of the war was very successful and runners
came and went as they
pleased.39 Purveyors were authorized to barter or trade cotton for
any medical supplies that were
aboard.40 Medicines, medical supplies, medical instruments, drugs
and pharmaceuticals were third to munitions and clothing as
contraband transported by blockade runners. Until the last of the
Southern ports
were captured by Federal troops, this avenue proved a very lucrative
and successful one. Fraser, Trenholm and Company, a Southern owned
trading business, became the premier blockade running business in
the Confederacy. During early 1863 alone, the company’s profits have
been estimated at $20 million dollars.41 The Army of Northern
Virginia was said to have been “dependent for chloroform, morphine,
quinine... almost entirely on the blockade runners” during the last
two years of the war estimated at $170,933 in Confederate
currency.42
Smuggling chloroform through Union lines to Confederate hospitals,
although officially declared illegal by both the government of the
United States and Confederate States, did occur. This “internal
trade” provided vast amounts of the much needed medical supplies,
declared contraband of war by the North, to the Confederacy. To make
this trade even more odd was the authorization, by the
Northern Congress, of Abraham Lincoln to trade with the South “ when
it seemed advantageous.”43 Southern Surgeon General Moore also
authorized Surgeon Richard Potts, a surveyor in the Western theater,
to trade with the North.44 By smuggling, the South was able to
maintain adequate supplies of chloroform, quinine and morphine.45
Perhaps this was inevitable - the states had traded freely before
the war and was a long established tradition. In exchange for the
required munitions, clothing and medicine, the South could provide,
on practically a daily basis throughout the entire war, the Northern
mills with cotton.46 Memphis, Tennessee was central to the “internal
trade” that occurred between the Union and the Confederacy. During
the Federal occupation of the city from 1862 to 1865, vast
quantities of supplies passed through Memphis. Despite the efforts
of Union officers to keep this trade under control, large amounts of
drugs were sent “southward” in exchange for cotton. The Union
Congressional Committee on the Conduct of the War, in July 1864,
estimated “that $20 million and $30 million worth of supplies have
passed through this city into the hand of the Confederacy.”47 Given
the need and desire to blockade the Confederacy by both land and
sea, it must have been exceptionally difficult to man both a 1000
mile long land border and a 3500 mile long sea coastline
effectively.
Another of the chief providers of medical supplies and chloroform to
the Southern armed forces were the Northern armies and the Northern
supply system! Although this method of procurement worked both ways
in the Civil War, the “Southern acquisition by this means were quite
noteworthy.”48 After
victories in battle, the Confederates would be able to help
themselves to the medical supplies left behind by the Union armies.
A North Carolina surgeon, following the Southern victory at Manassas
on 21 July 1861, told of the seizure of “a large number of cases of
fine surgical instruments and a large stock of medicines... [the
medical staff would] not be troubled in this line of preparation for
another action.”49 This, however, was only one of two ways the
Confederate troops “drew rations” from Northern suttlers - raiding
Union lines proved a frequent and valuable source from the beginning
until the end of the war. During
General Thomas J. Jackson’s Shenandoah Valley Campaign, May-June
1862, his troops captured 15,000 cases of chloroform.50 He went on
to pillage Union General John Pope’s supply depot at Manassas
Junction on 27 August 1862.51 During September 1862 yet another
large haul of medicines, instruments and other medical supplies was
reported from the Kanawha Valley, estimated at $20,000. One huge
cache, appropriated by General Nathan Bedford Forrest’s cavalry,
occurred during a raid in Western
Tennessee. After requisitioning what his immediate command needed
from the three wagons, Forrest shipped the remainder to Atlanta.
There a medical purveyor appraised the value of the goods at
$150,000 in gold.52 As late as September 1864 found Confederate
raiding parties commandeering the food and supplies they needed. In
a sortie from their siege lines at Petersburg, Virginia, Confederate
cavalry raided the Union supply, returning with over 2400 cattle and
11 wagons.53 No reference is made of the contents of the wagons and
one must speculate as to the details of the goods captured. If one,
however, recalls the top three items of need: munitions, clothing
and medical supplies, one may surmise what was considered of value
and what was contained in the wagons.
Reports from
Confederate sources also show that the dearth of the supply of
medicines was not entirely true. The primary consistent complaint of
shortages involved medical instruments.54 The Confederate drug
situation may have been slightly exaggerated. Stewart Brooks writes
“some prime sources relating to the subject are far from emotional,
a few going so far as to deny the problem was ever what might be
called desperate - especially in regard to chloroform.”55 The
conclusion of a Master’s Degree thesis by Charles F. Ballou, II is
that Confederate hospitals in and around the Richmond hospitals were
prevented from the acute need of medical supplies by dedicated
purveyors until the end of the war.56 Accounts from field hospitals
report shortages as well as an abundance of supplies. One
description mentions such an overabundance that surplus medications
could be sent to a colleague from home. “I have more of it than I
could use in two years.”57 J. Julian Chisholm, an outstanding
purveyor, brilliant medical author and surgeon and inventor
of medical equipment, was an outstanding administrator. Through his
pains and tireless efforts, hospitals in the Richmond area never
seemed short of supplies. “In assuring that imported medical
supplies from blockade runners reached the lines of action, he had
no peer.”58 Another writes “Normally, we were scant of medicines,
and generally, they were the commoner kinds. At times, however, we
were well supplied, and with excellent preparations,” the latter
following capture of Union supplies or after receiving goods through
purveyors from blockade runners. “Normally we were short [but] at
times we were well supplied.”59 H. H. Cunningham writes “... some
Confederate medical officers have gone so far as to state that at no
time during the struggle did they fail to have a sufficient quantity
of the essential needed.” Surgeon Deering J. Roberts found many
Southern doctors “always had an abundant supply of quinine, morphine
and chloroform - the most important drugs of all.” The sick and
wounded of Petersburg, site of a 10 month siege at the very end of
the war, “did not suffer for anything necessary to their comfort.”
Surgeon General Moore, in a report to the Secretary of War, dated
February 1865, stated that his department had a limited amount of
some supplies and over a year’s worth of others. Moore believed that
if the department were allowed to retain the skilled staff they
currently possessed at the various laboratories and purveying depots
and were allowed to import medicines through the lines in
Mississippi and Alabama, the sick and wounded would not suffer for
want of the essential medical supplies.60 The appearance of
shortages began in early 1864. A memorandum to the Surgeon General,
in March 1864, reported a list of 39 medicines removed from the
supply table. Chloroform and opiates, significantly, were not on
this list.61 Shortage notices also increased as the Confederate
transportation system collapsed near the end of the war. Needed
supplies arrived “tardily at their destination. Until near the end
of the war, however, the Medical Department was reasonably
successful in supplying its patients with the necessary medical
supplies, assisted in these undertakings by state and private
efforts.62
CONCLUSION
If, in the end, the doctors in gray and butternut were reasonably
well stocked with medical supplies and in particular, chloroform,
why was there such a great push so early in the war for the search
for indigenous alternatives? Very few people on either side believed
the war would last long; in 1861 both North and South thought the
other would back down from their respective positions and the
fighting would cease with the successful conclusion for their side.
Most experts could not conceive that the war would last four long
years. The drive to explore the use of home grown plant substitutes
for traditional medicines and drugs seems to be part of a general
movement to establish self sufficiency. Southern self-sufficiency
meant just that - independent means for an independent sovereign
nation. In this respect they proved successful thanks, in part, to
the writings of Surgeon Francis Perye Porcher.
Although indigenous
botanical substitutes were used by the South, they were primarily
used for purposes other than anesthesia. The Southern pharmaceutical
industry, nonexistent at the start of the war, became an adequately
proficient part of the Confederate medicinal supply system. Blockade
running, until the final ports were closed, furnished the South with
quantities of European medicines. The thriving “internal trade,”
although officially banned bilaterally, provided the Confederate
armies with another source of medical supplies. Lastly, the Federal
army itself contributed vast amounts of medical supplies and
medicines to the Southern cause. In spite of the eventual collapse
of the Confederate transportation system, field and general
hospitals generally possessed adequate amounts of the medicine that
they considered essential: chloroform, quinine and opium. The only
genuine shortage for which there was a universal complaint was the
lack
of medical and surgical equipment. The Southern medical cause was
fortunate for they enjoyed the exertions of men like Surgeon General
Samuel Preston Moore, Surgeon J. J Chisholm and Samuel Hollingsworth
Stout63 whose innovative techniques and administrative efforts kept
both the field and general hospitals stocked with the medicines that
were considered essential at
that time. Thanks to their combined efforts the Southern military
hospitals were not dependent on indigenous botanical substitutes for
anesthesia nor did they go without essential basic medical supplies.
Compared to the ability of the other aspects of the Southern supply
system to supply munitions, clothing and forage - from the beginning
to the end of the American Civil War the Confederate States Medical
Department provided outstanding medical support for her fighting
soldiers.
ENDNOTES
1. J. Julian Chisholm, A Manual of Military Surgery for the Use of
Surgeons of the Confederate States Army, Columbia, Evans and
Cogswell, 3rd edition, 1864,
p. 426.
2. Ibid., pp. 221-225, p. 416, pp.426-430. Confederate States
Medical and Surgical Journal, January 1864 - February 1865, as
noted by a variety of assorted
case studies throughout the Journal.
3. Chisholm, (n.1) Manual of Military Surgery, p. 427.
4. Ibid., p. 427.
5. H. H. Cunningham, Doctors in Gray: The Confederate Medical
Service, Gloucester, Massachusetts, Peter Smith, 1970, pp.
148-149. Reprinted from 1958 edition, Louisiana State University
Press.
6. Charles F. Ballou II, Hospital Medicine in Richmond, Virginia
During the Civil War: A Study of Hospital No. 21, Howard’s Grove and
Winder Hospitals, Blacksburg, 1992, p. 96.
7. Francis Perye Porcher, A Sketch of the Medical Botany of South
Carolina, Philadelphia, T.K. and P.G. Collins, 1849 and The
Medicinal, Poisonous, and Dietetic
Properties, of the Cryptogamic Plants of the United States, New
York, Baker, Godwin, and Co. 1854.
8. Cunningham, (n. 5) Doctors in Gray, p. 149.
9. U.S. War Department (comp.) War of the Rebellion: A Compilation
of the Union and Confederate Armies, Washington, D.C., 1880-1902
Ser. IV, Vol. II, 13,
quoted in Ballou, Hospital Medicine, p. 97.
10. Francis Perye Porcher, Resources of the Southern Fields and
Forests, Medical, Economic and Agricultural, Charleston, Steampower
Press of Evans and Cogswell, and Richmond, Virginia, West and
Johnston, 1863, as reported in the preface during a 1950s reprint of
the book. Subsequent searches have failed to locate any of the books
exactly as listed, however, a text of
similar title was located and may be one to which the writer
referred: John Bachman, An Inquiry into the Nature and Benefits of
an Agricultural Survey of the State of South Carolina, Charleston,
Miller and Brown, 1843.
11. Time-Life Books, The Civil War Series, Twenty Million Yankees,
Alexandria, Virginia, 1986, p. 73.
12. War of the Rebellion, (n. 9) Ser. I, XIX, II, 614, quoted in
Ballou, (n.6) Hospital Medicine, p. 99. Cunningham, (n. 5) Doctors
in Gray, p. 158.
13. Medical and Surgical Journal, (n.2) Vol. I, No. 7, 107.
14. Ibid., pp. 107-108.
15. Dr. Bartholomew Egan held that opium from white poppies was
equally as good as the commercial product. Porcher asserted that
there were no fatalities from the use of locally produced
chloroform. Quoted from
Cunningham, (n. 5) Doctors in Gray, pp.150-151.
16. Medical and Surgical Journal, (n. 2) Vol. I, No.3, 38.
17. Ibid., Vol. I, No. 7, 38.
18. Ibid., Vol. I, No. 6, 84-86.
19. Cunningham, (n. 5) Doctors in Gray, p. 150.
20. Ibid., p. 150.
21. Stewart Brooks, Civil War Medicine, Springfield, Illinois,
Charles C. Thomas, 1966, p. 70.
22. Time-Life Books, The Civil War Series, Sherman’s March,
Alexandria, Virginia, 1986, page 108. Porcher, Southern Fields.
There appear to be two editions of this book, one of 601 pages and
the other of 594 pages.
23. Porcher, (n. 7) Southern Fields, p. 197.
24. Ibid., p. 417.
25. Ibid., p. 475.
26. Ibid., p. 44. In order to evaluate the efficacy and action of
the drug, Porcher frequently perfomed tests of the plant substitute
on himself.
27. Ibid., p. 44.
28. Ibid., several listings throughout the text.
29. Cunningham, (n. 5) Doctors in Gray, p. 150. Medical and Surgical
Journal, (n. 2) Vol. I, No. 6, 84-86.
30. Wyndham B. Blanton, M.D., Medicine in Virginia in the Nineteenth
Century, Richmond, Virginia, Grant and Massie, Inc.,1933, page 286.
31. Chisholm, (n. 1) Manual of Military Surgery, p. 426.
32. Ballou, (n. 6) Hospital Medicine, p. 100.
33. Chisholm, (n. 1) Manual of Military Surgery, pp. 427-428.
34. Hunter McGuire, M.D., “Account of the Wounding and Death of
Stonewall Jackson,” The Virginia Medical Monthly, 1961, Vol. 88,
No. 10, 5, originally printed in the Richmond Medical Journal, 1:403
May, 1866.
35. Chisholm, (n. 1) Manual of Military Surgery, pp. 428-429. Susan
Provost Beller, Medical Practices in the Civil War, Cincinnati,
Ohio, Betterway Books,1992 page 72. A scale illustration of the
inhaler is on page 74.
36. Ballou, (n. 6) Hospital Medicine, p. 96. Brooks, (n. 21)
Medicine, p.69. Time-Life, (n. 22) Sherman, p. 108.
37. Cunningham, (n. 5) Doctors in Gray, p. 148. Norman H. Franke, an
able student of
Confederate pharmacy, feels that the military failed to make full
use of the skilled druggists in the South.
38. Cunningham, (n. 5) Doctors in Gray, p. 147. Taken from a direct
quote of Mohr.
39. Beller, (n. 35) Medical Practices, p. 67. Time-Life Books, The
Civil War Series, The Blockade, Alexandria, Virginia, 1986, pages
86-101.
40. Ballou, (n. 6) Hospital Medicine, p. 98. Frank Reed Freemon,
Medical Care During the American Civil War, Ann Arbor, Michigan,
U.M.I, 1992, pp. 107-108. Glenna Ruth Shroeder-Lein, Waging a
War Behind the Lines: Samuel Hollingsworth Stout and Confederate
Hospital Administration in the Army of Tennessee, Ann Arbor,Michigan,
U.M.I, 1991, pp. 76-77.
41. Time-Life, (n.39) Blockade, p. 98.
42. Cunningham, (n. 5) Doctors in Gray, p. 135.
43. Brooks, (n. 21) Medicine, pp. 67-68.
44. Cunningham, (n. 5) Doctors in Gray, pp. 136-137. From a direct
communication from Moore to the Confederate Secretary of War.
45. Beller, (n. 35) Medical Practices, p. 78.
46. Time-Life Books, (n. 11) Yankees, pp. 73-75. 34. Cunningham, (n.
5) Doctors in Gray, p. 137.
47. Cunningham, (n. 5) Doctors in Gray, pp.136-138.
48. Ibid., page 139.
49. Ibid., page 139.
50. James M. McPherson, Battle Cry of Freedom, New York, New York,
Balantine Books, 1988, page 487. Cunningham, (n. 5) Doctors in Gray,
p. 139.
51. Time-Life Books, The Civil War Series, Lee Takes Command,
Alexandria,Virginia, 1986, pp. 129-130.
52. Cunningham, (n. 5) Doctors in Gray, p. 139.
53. Time-Life Books, The Civil War Series, Death in the Trenches,
Alexandria, Virginia, 1986, pp. 111-115.
54. Cunningham, (n. 5) Doctors in Gray, pp. 156-159. Ballou, (n. 6)
Hospital Medicine, pp. 96-98.
55. Brooks, (n. 21) Civil War, page 67.
56. Ballou, (n. 6) Hospital Medicine, pp. 96-108.
57. Spencer G. Weich, A Confederate Surgeon’s Letters to His Wife,
New York, 1911, p. 131, quoted in Ballou, (n. 6) Hospital Medicine,
p. 100.
58. F. Terry Hambrecht, “The Missing Letters, Insights into the
Confederate Medical Department,” The Maryland Line, Baltimore,
Maryland, 1991, II, 2, quoted in Ballou, (n. 6) Hospital Medicine,
p. 98.
59. Taylor: De Quibus: pp. 302, 316, 318, 319, 320, 330, quoted in
Blanton, Medicine in Virginia, (n. 30) pp. 278-279.
60. Cunningham, (n. 5) Doctors in Gray, pp. 159-160.
61. National Archives, DXLVII, 182, quoted in Ballou, (n. 6)
Hospital Medicine, pp. 106-107.
62. Cunningham, (n. 5) Doctors in Gray, pp. 161-162.
63. Shroeder-Lein, (n. 40) Stout, iii. Surgeon Stout was by 1863 the
Medical Director of Hospitals for the Confederate Army of Tennessee,
supervising as many as 60 hospitals in Tennessee, Georgia, Alabama
and Mississippi. Proficient at personnel management, he oversaw all
aspects of medical care in this vast area, made more difficult
during the later years of the war with
Union advances and a crumbling Confederate transportation system. |