Transfusions
During the Civil War
Prior to the use of cross-typing of
blood groups to determine A, AB, O compatibility
From the Medical and Surgical
History and the Geo. Tiemann Catalogue 1870's
GEO. TIEMANN & CO.'S
SURGICAL INSTRUMENTS,
TRANSFUSION.
Fig. 211.—Fryer's
Transfusion Apparatus.
(Extracted from the
Medical & Surgical Record,
April 15, 1874.)
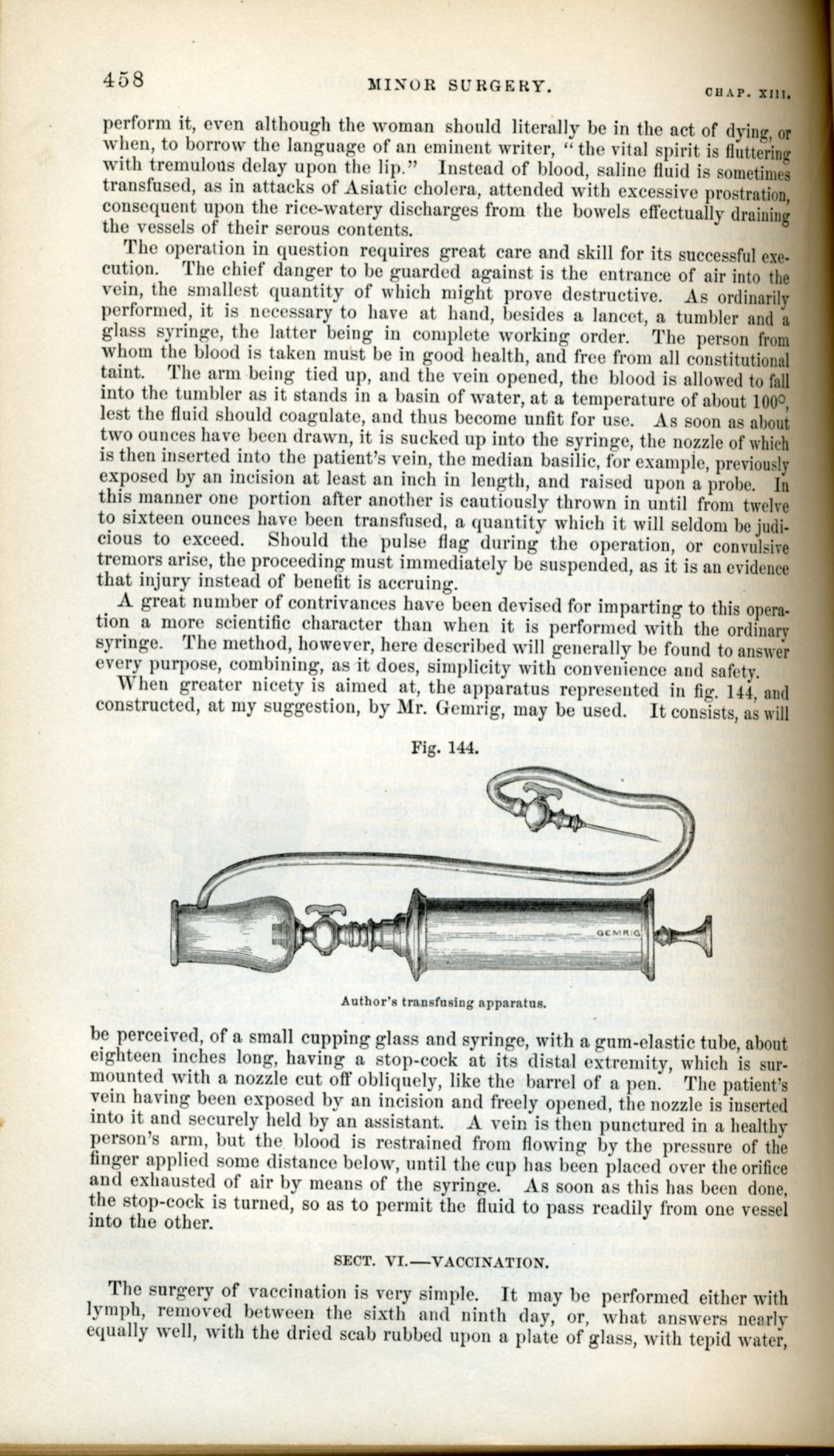
A few remarks on the
Transfusion
of Blood, with a
modification of the
Apparatus of Aveling. By
B. E. Fryer,
M. D., Surgeon U. S.
Army. post-Civil War
To show that the subject of
transfusion
is one which a large portion
of the profession has not
yet fully weighed the
importance of nor realized
the fact that this measure
can frequently be made
applicable in cases which
are now quietly otherwise
yielded to death, we have
only to call attention to
the rarity of reported
instances (see below
examples) in which the
operation has been taken
advantage of, and refer to
the many obvious ones in
which it should be made
available. Even in
threatening dissolution from
the direct loss of
blood,—such as from wounds
of large vessels, from
prolonged epitasis, or, in
probably one of the most
frequent opportunities met
with, from hemorrhage,
post-partum, where the
restoration of blood by
transfusion
has been, so to say,
legitimatized—but few of us
are prepared for the
emergency, or if prepared,
do promptly act and give the
then affected only chance of
life.
We will briefly state the
kind of cases in which it
has occurred to us that
transfusion
should "be had recourse to
without hesitation, and they
may be conveniently note
under two headings.
We would include in the
first class those cases
in which a copious
blood-loss has occurred and
immediate death is
threatened. As is well
known, it is in these mainly
that the measure lias been
applied. It might well be
tried in coses of injury
accompanied by a more
moderate hemorrhage, and
where it is necessary to do
an important surgical
operation, and this
operation is delayed (often
disastrously) for a reaction
by ordinary means. Moreover,
it should be done before or
aftor necessary surgical
measures in the astheuic
patients, fu order to avoid
pytrmia and its allied
evils, especially in
operations where the
peritoneum is involved.
After labor, too, where
hemorrhage may have been
great, but not enough to
threaten immediate death, it
should be done to avoid
septicemia difficulties. For
that depression from the
loss of blood is a most
direct cause of pyemia and
its pathological associates,
those of us who have had to
treat large numbers or
gunshot and other injuries,
and to operate In these
cases, where hemorrhage and
other depressing causes had
done sad havoc, well know.
But we have in the second
class a larger number of
cases—diseases both acute
and chronic—and bore we more
commonly meet with
opportunities. In such,
transfusion
has scarcely
been thought of; but it is
in these, too, it ought in
be, and will
Ims, wo think, taken
advantage of. Of the acute
cases we refer to, those in
which natural nutrition is
for the time suspended,
either from a direct lesion
of the blood-making system
in one or more of its
divisions, or is indirectly
affected in consequence of
some profound systemic
impression, where if we can
but bridge over a short
period by keeping life's
machinery goin^. we niay
ultimately bring about a
restoration of the healthy
nutrition process, and thus
save life. To particularize
: acute gastric troubles,
giving excessive and
continuous vomiting; acute
diarrlneas and dysenteries;
in peritoneal intluiinuatUms,
in some of the low forms of
fevers where waste is
excessive mid the*
absorption of nourishment
nti. In cholera it
should be done more
generally than it has been.
It might In tried, t"<> in
sonic of the acute diseases
of young children,
particularly ill those'
which give convulsive
movements and convulsious
proper, and which often
indicate to us diminished
blood-supply to the brain,
and tell us that death can
again put the nerve-centers
quietly at work.
In chronic eases where the
blood-making is reduced or
nearly destroyed, we might
often prolong life by
transfusion. Such cases are
not frequent, though we need
not enumerate them. We might
well apply the measure even
in some cases of phthisis pulmoimlis.
In regard to the fluid to be
transfused. As is well
known, human blood is that
to be, most desired, after
the blood of some of the
lower animals may be
selected. Hutlder, of
Canada, threw into the veins
of some of his cholera
patients fresh milk, and
with excellent results. The
writer has experimented with
milk injections in the veins
of (logs, and though the
experiments have not been
completed as to a test of
the nourishing effects of
the milk so given, no bad
symptoms have become
apparent. If it can be
satisfactorily proved, that
milk may be safely and
generally used in
transfusion, and with the
desired result, a great
advance will
Iks mode in the
matter, it being nearly
always obtainable, while
many of the difficulties and
inconveniences in the use of
blood will be avoided. A
saline solution (such as
that of Mr. Little*) should
be tried to save life, if
nothing else is at hand.
The instruments for
transfusion
are to us is well
known, quite numerous, and
while many of them are very
good, we believe that of Aveling,
for immediate
transfusion,
to be probably the simplest,
safest, and most easy of
application. We have lately
modified it by adding
another bulb to the tube,
and by having both tube and
bulbs cost of the rubber
into one piece. By the
additional bulb we can save
time in doing the operation,
and can keep the blood
moving along the tube almost
continuously. In having the
ruin- and bulbs in one, we
do away with the metal portions which couples
them in Aveling's apparatus,
and we thereby diminish the
risk of blood lodging and
coagulating; while we if necessary, compress the
whole apparatus more
completely. As in Dr. Aveling's instrument, there
are no valves.
The instrument of Aveling is
intended for immediate
transfusion. We have added a
glass vessel which can be
fitted to the tube, and the
whole then used as a mediate transfuser if desired. The
accompanyiug cut gives a
good representation of the
apparatus.
The manner of using the
instrument Is very similar
to Aveling's. The canula
marked S is placed in
the giver's vein, that
marked in the vein of the
receiver. The tube and bulbs
having been filled with warm
water. or better, with Mr.
Little's saline solution
(also warm), are now
adjusted to the canulas and
the blood allowed to flow
into the apparatus. The
canula being steadied by an
assistant, the tube is to be
nipped tightly between the
fingers, close to the
giver's or efferent end, and
then the bulb marked 1 is to
Ite compressed, and the
lilood of course forced on
towards the receiver. While
this bulb is still held
compressed, the tulie at the
giver's side is to bo
relaxed, and that portion of
it between the bulbs is to
be nipped; bulb 1 is
relaxed. a.nd No. 2
compressed and held then the
tube at the receiver's side
is to he seized and held to
prevent regurgitation, and
the whole apparatus allowed
to refill. The same
operation to be repeated
till sufficient blood is
transfused. As suggested bv
Dr. Aveling, a few drops of
ammonia solution may
be
injected into the
bulbs now and then, by a
fine-pointed hypodermic
syringe, in order to more
effectually prevent
coagulation. It will be
found that considerable
force is necessary in
sending blood or other
fluids into the veins. This
we discovered while doing
transfusion
twice in a case
after hemorrage from gunshot
injury, and we have also
found it in our experiments
on the lower animals. It is
a fact that we nave not seen
noted in connection with
transfusion,
and one well worth
remembering.
In order to age the
apparatus as a mediate
transfuser, the vessel
marked A in the cut
receives the blood, the tube
is to be applied, and the
instrument used as before
directed. If the blood is not deflibrinated
and strained, three or four
drops of ammonia solution are added, in order
to avoid coagulation.
The instrument is made bv
Messrs.
George Tiemann &,
Co., 67 Chatham Street,
New York.
We would suggest to those
who may become interested in
transfusion, that though the
operation is a simple one.
it requires care, and it
should first 'be practiced
once or twice on the lower animala no difficulty will
then be had in doing It on
man when occasion requires.
Fig. 212.—Garrigue's
Mediate
Transfusion
Apparatus.
Draw eight or ten ounces of
blood from a healthy person
into a clean vessel, whilst
it is accumulating whip it
with a silver fork, a stick
of wood or a bunch of straw,
then strain it through a
piece of cleanly washed
linen into a vessel placed
within another containing
warm water (about 105 C.)
Warm the syringe, put the
suction end A into
the blood, compress the
bulb, and when it flows
through the canula, turn the
stopcock C.
Having bared the patient's
arm, raise a fold of skin
over a vein at the bend of
the elbow, divide it and
pass a probe or thread under
the vein thus brought into
view. This is now held with
a pair of forceps or
tenaculum and an incision
made with a lancet or pair
of fine pointed scissors,
carefully avoiding to wound
its posterior wall. Now
introduce the canula D,
open the stopcock and
inject slowly.
The bulb contains about
three fluid drachms, but by
moderate compression about
two only are expelled. In
most cases it suffices to
inject from four to six
ounces. If resistance, not
due to external pressure be
felt, or dyspnoea, or any
other untoward symptom
appear, the operation has to
be interrupted or ended.
Dress the wound as after
phlebotomy.
After use, the instrument
must be thoroughly cleansed,
which is best done by
separating all the parts and
washing them in warm water.
A transfusion technique from
Samuel Gross's Operative
surgery book:

|
|
Medical/Surgical
History--Part III, Volume II
Chapter XII.--Wounds And Complications.
Treatment of Haemorrhage.
Two cases of
transfusion
of blood are found on the records; one, a successful operation, was
performed by Surgeon E. Bentley, U. S. V.; the other, a fatal case,
by Assistant Surgeon B. E. Fryer, U.S.A. Both are here detailed:
CASE 1186.--Private G. P. Cross, Co. F, 1st Massachusetts Heavy
Artillery, aged 19 years, was wounded in the right leg, before
Petersburg, June 16, 1864, and entered the Grosvenor Branch
Hospital, Alexandria, two weeks afterwards. Surgeon E. Bentley, U.
S. V., who operated in the case, made the following report:' "The
injury consisted of a flesh wound on the posterior aspect of the
leg. At the date of the patient's admission he was exsanguineous
from previous loss of blood. Owing to his condition no operative
measures were adopted, but his languishing vital powers were
sustained by stimulating treatment combined with highly nutritious
diet. Under this method he slightly improved in strength, but the
circulating fluid was so impoverished in quality and reduced in
quantity that the face of the wound looked pale and bad, and
ultimately, on August 12th, it assumed a gangrenous aspect. Local
applications, such as creasote, charcoal poultices, nitric acid,
etc., were applied to combat this condition. These means failed to
arrest its onward progress, the leg presenting in a short space of
time a mass of gangrenous sloughs, horribly fetid. Haemorrhage from
the posterior tibial artery again commenced on the afternoon of
August 15th, when it was deemed advisable to amputate to prevent
further loss of blood. The operation was accordingly performed just
at the tubercle of the tibia, the condition of the parts not
allowing a flap to be made below that point. Not more than two
tablespoonsful of blood was lost; but the patient not seeming to
rally, it was determined to test the method of transfusion of blood
as recommended by Brown-Séquard. Blood having been obtained from the
temporal artery of a strong healthy German, an attempt was made to
penetrate the internal saphenous vein, but was unsuccessful on
account of its small size; after which an <ms_p3v2_812>opening was
made into the median basilic, and about two ounces were transfused
by means of a Tiemann's syringe. Immediately after the injection a
marked difference was noticed in the patient's pulse, which became
stronger and firmer. He was then removed to his bed and generous
diet was administered, together with stimulants and tonics, under
which treatment he gradually improved, his appetite became better,
his strength increased, and the stump assumed a healthy aspect. On
October 20th the stump had healed and the patient had so far
improved as to be able to be furloughed. At its expiration he
returned, and, finally, he was transferred to Webster Hospital,
Manchester, January 13, 1865, cured." The patient was ultimately
discharged from Central Park Hospital at New York City, June 9,
1865, and pensioned, and afterwards he was supplied with a "Hudson"
artificial limb. This pensioner died August 24, 1867.
CASE 1187.--Private J. Mort, Co. E, 105th Illinois, aged 37 years,
received a flesh wound in the upper third of the left leg, at
Keneeaw Mountain, June 26, 1864, by a musket ball, which lodged
between the tibia and fibula. He entered Brown Hospital, at
Louisville, nine days after receiving the injury, the missile having
been extracted and the wound looking unhealthy and sloughing.
During.the night of July 24th the patient had a copious haemorrhage
from what was supposed to be the anterior tibial artery, which was
arrested. On July 26th bleeding again commenced, the blood welling
up from between the bones and from the tissues posterior to them. It
was then deemed necessary, in order to save life, to amputate, which
was done through the upper third of the leg by the circular method,
by Assistant Surgeon B. E. Fryer, U.S.A. Ether was used as an
anaesthetic, and three ligatures were applied, the patient reacting
very slowly. On the following day it was determined to transfuse
some blood into the patient, for which purpose, in the absence of
any other suitable apparatus, an ordinary gutta-percha syringe was
used, the nozzle of which was filed to fit a small tube having a
stop-cock through its centre. The right cephalic vein having been
selected, an opening was made carefully into it, and the syringe
having been warmed and filled with blood from a healthy man, a
little of which was allowed to flow from the syringe before forcing
its nozzle tightly into the tube in order that any air might be
driven out, the tube was introduced and the stream of blood was
slowly and carefully forced in. About sixteen ounces were thus
transfused. The first effect upon the patient was to increase
respiration from about fifteen to twenty-eight per minute, though it
soon returned to its normal number of about sixteen. The pulse ran
up from one hundred to one hundred and thirty, which, however, also
soon returned to what it had been. The man's general condition was
greatly improved. His pulse became fuller and slower; he slept well;
his stomach retained food, and altogether the prognosis became more
favorable. On August 4th haemorrhage commenced from the face of the
stump, the whole surface of which appeared to be involved. From the
effects of this, and from chronic dysentery, the patient died on the
following day, August 5, 1864; although his condition, from the
effects of chronic dysentery and of the haemorrhage at the time of
the transfusion,
was such as hardly to expect his recovery, the improvement was such
as to show that the operation was not only justifiable, but that it
was to all intents a success. The history of the case was reported
by the operator.
| |